


10. Silence on the surface: how toxic relationships within a team jeopardise diving safety
A calm before the storm: how toxic team dynamics threaten diving safety before anyone even enters the water
In the first week of June 2026, the world’s first dedicated conference on human factors in diving took place on the island of Vis in Croatia. The article below explores this topic, addressing the issue of how isolated diving operations can become totalitarian institutions, how being powerlessness to communicate and how desperation under such conditions, can lead to very negative poor behaviours, and whether a culture of fair treatment offers a solution.

I wanted to depict the slow process that leads to learned helplessness, to acts of desperation, to reactions to recurring situations that not only sap motivation, the willingness to cooperate, and the drive to improve. A sense of helplessness and powerlessness, yet at the same time resistance and a reluctance to give in. Why is it that sometimes creating a real threat or pushing beyond what seem to be the ultimate limits of mutual cooperation may not be an individual’s choice, but rather the result of their relationship with the organisation and the team? Behaviours that cause harm, put people at risk, and damage operations may be the result of ignored voices, team dynamics and neglect, which mean that at a given moment – even if it may seem irrational – such behaviour becomes the only final cry for change
The room you never see
When guests arrive at the dive centre, they see what’s on the surface: smiling staff, ready equipment, a professional briefing. Guests judge safety based on what they can see. And what they see looks fine.
However, they cannot see what is happening behind the scenes. Has the divemaster had a good night’s sleep? Did the junior instructor mention the current at yesterday’s dive site – and did anyone listen to him? Are the dive supervisor and the boat captain still not speaking to each other following an argument two weeks ago, which officially never took place?
We devote a great deal of effort to analysing the human factors directly related to diving. Decision-making under pressure. Situational awareness. Communication between dive partners. All of this matters. However, the conditions that lead to failure – or ensure safety – are almost always determined above the surface, in interactions that take place before anyone even enters the water.
The space we rarely talk about is the briefing room before the briefing itself. The kitchen at 6 am. A WhatsApp group at midnight. Interpersonal relationships, tensions, unresolved misunderstandings. Instructions or feedback were delivered in the wrong tone when everyone was already tired. Cynical remarks, personal animosities that came across a few notches too sharply.
Why closed environments are different
A safari boat. A dive centre on an island. A seasonal base where the same group of people work, eat and sleep together for many months on end. Sociologist Erving Goffman called these ‘total institutions’ – spaces where work, rest and social life merge within the same physical environment, with the same people, and without the possibility of returning home after a shift ends.
In a normal workplace, you can process a difficult conversation from the previous evening during your morning commute. In a confined environment, that conversation stays with everyone right up until dinner. The tension from Monday’s briefing is still palpable on board on Friday. The hierarchy that determines who has precedence in safety decisions is the same hierarchy that decides who gets the better cabin and who does the washing-up.
Proximity and duration amplify everything. They also mean that things become invisible more quickly – because when there is no external point of reference, ‘the way things are here’ simply becomes the way they are.
How what is normal becomes toxic
The most important thing to understand about toxic team dynamics in diving operations is that they do not require bad people, unsuitable personalities or difficult relationships. They are based on ordinary people in ordinary situations, subject to three mechanisms that exist in every team – but which operate with extraordinary intensity in a confined environment.
The authority gradient. In expert communities, a hierarchy naturally forms around certifications, experience and the number of dives. This is functional. It becomes dysfunctional when the gradient becomes so steep that information stops flowing upwards. When a junior divemaster notices something — a guest struggling, faulty equipment, a plan that doesn’t allow for extra time for a briefing or filling additional tanks — but doesn’t speak up, because their accumulated experience working there has taught them that speaking up about such things comes at a price. Helmreich’s research into team resource management in aviation directly demonstrated this pattern: steep authority gradients correlate with uncorrected crew errors. The junior crew member knew. The junior crew member said nothing.
Normalisation of deviation. Diane Vaughan identified this process whilst investigating the Challenger disaster, and it operates in diving operations with quiet efficiency. The standard is bent once. Nothing happens. It is bent again.
Nothing happens. Over time, the distorted standard becomes the new norm. The team loses the ability to recognise its own anomalies, as they have become part of everyday life. The most dangerous phrase in any diving centre: ‘That’s just how we do things here’.
Chronic interpersonal stress. When relationships within a team are constantly strained – not in a catastrophic way, not in an obvious way, but simply chronically – staff struggle daily with a cognitive load that takes precedence over all diving-related demands. Research on stress and decision-making is consistent: chronic interpersonal stress narrows attention, impairs working memory and slows down situational assessment in ambiguous circumstances. A Divemaster who hasn’t slept because he ‘had to’ entertain guests late into the night. An instructor who avoids eye contact with the manager during the pre-dive briefing. They stand at the water’s edge already at a disadvantage. No one measures this deficit. No one factors it into the dive plan. But it is there, shaping every subsequent decision.
Five stories
What does it look like when someone stops believing that this still makes sense? It doesn’t look like a dramatic departure from the norm. It isn’t foreshadowed.
Loss of initiative. At a small diving centre, the task of filling tanks was shared between two staff members. The person responsible for filling tanks in the afternoon also acts as a guide and instructor. During the high season, this means skipping lunch, rushed briefings and constantly having to step away from the compressor. This issue is raised with the management. A decision is made – the person who had previously been filling tanks in the morning will also take on the afternoon shift. No one asks this person if they agree to this. The person who has been given these new responsibilities protests. Repeatedly. And then, one afternoon, they do not fill the tanks. Guests arrive. The boat is ready. There is no air. Negligence? Sabotage? Or perhaps the only language left to someone who had run out of words?
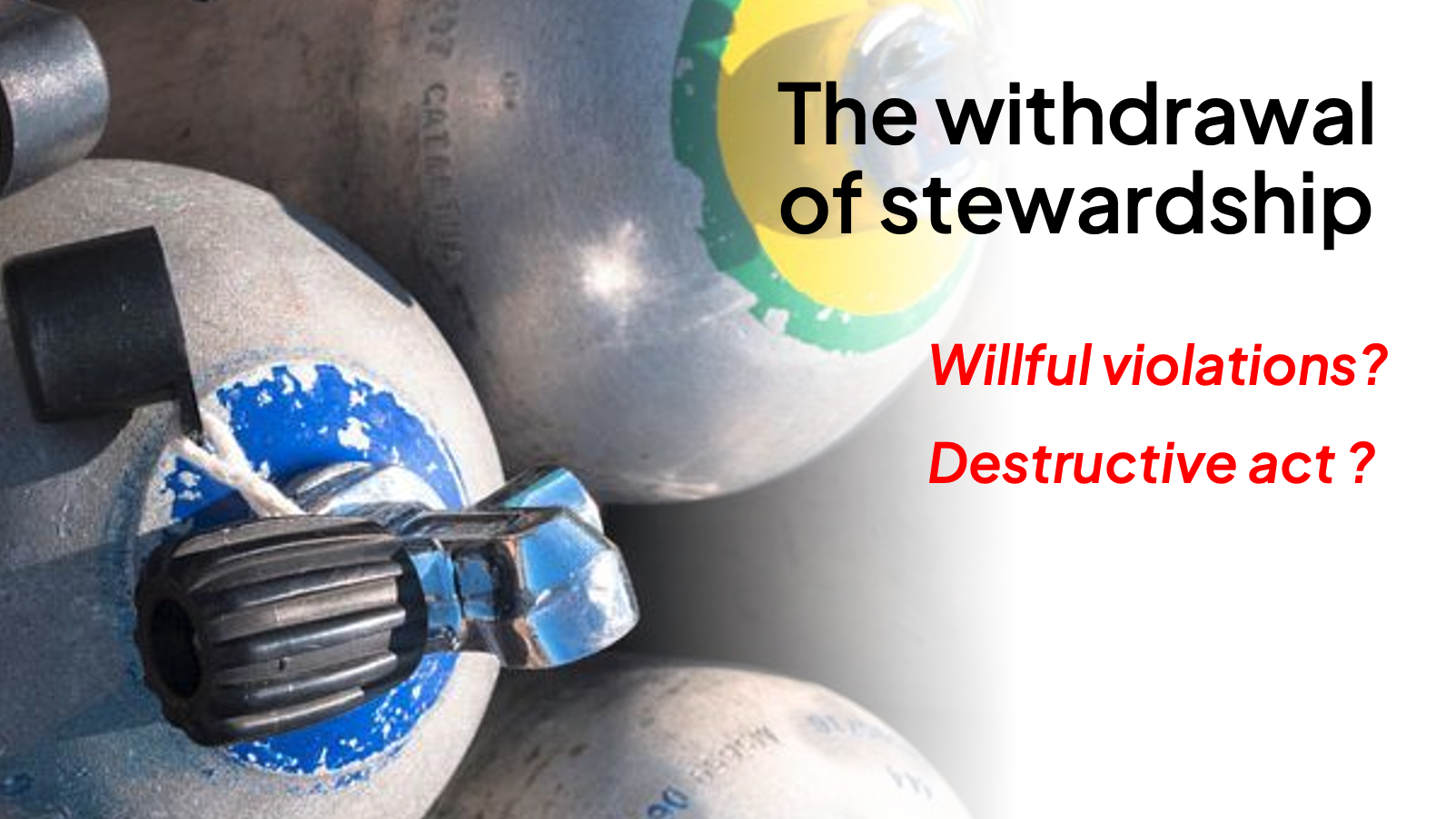
Withdrawal of stewardship. A new instructor at the diving centre points out that it is very easy to confuse full tanks with empty ones. He suggests a solution: set the filled tanks aside and label them clearly. The idea is accepted. However, nobody puts it into practice. So the person who suggested it does it himself, every day. Everyone quickly gets used to where and how the full tanks are labelled. This helps to avoid many mistakes. One day, the person who had been doing this work – which other staff were also supposed to do – becomes frustrated and stops. No one supported her; no one else did it; everyone simply benefited from it. The cylinders are issued as full, but it turns out they aren’t once the guests are already on the boat. In the language of human factors: failure to correct errors. In the language of blame: wilful negligence. The same act. Different language. Different consequences for the person involved.
Return of responsibility. The instructor observes the condition of the regulator sets deteriorating. He repeatedly asks for service kits. The manager is consistently uninterested — what we have is fine. The regulators break down one after the other. Eventually, one of the guests needs a replacement. The divemaster tries out more regulators. Each one fails. They lead the guest to the manager’s office: ‘I’ve got no working regulators left. So please, sort this out with this gentleman; the boat leaves in 10 minutes.’ In the language of human factors: restoring the structure of responsibility. In the language of a violent organisation: ‘Acting to cause harm’.

Demonstration. The instructor tries repeatedly to explain to the new helmsman that switching off the engine before securing the lines poses a real safety risk. The helmsman dismisses this every time: “I always do it this way.” One day, when the stern line is already secured but the bow line is not, the engine is switched off. The instructor is standing on the jetty. The bow line is thrown towards him. He fails to catch it. The bow drifts. The engine has to be restarted. Words have ceased to have any effect. Instead, consistency was chosen.
Transfer. A certified diver has obvious buoyancy problems on numerous dives — he sinks, stirs up sediment, ignores advice. He asks for a larger, heavier steel cylinder. The instructor warns him again: “You’re already overloaded.” The diver replies: “I’m diving fine, I need more weight for the bigger cylinder.” During the next dive, the instructor watches as the diver drifts away from the group, sinking to a depth of twelve metres. And waits. He intervenes at a depth of thirty-five metres, where the diver is standing on the seabed, unable to ascend.
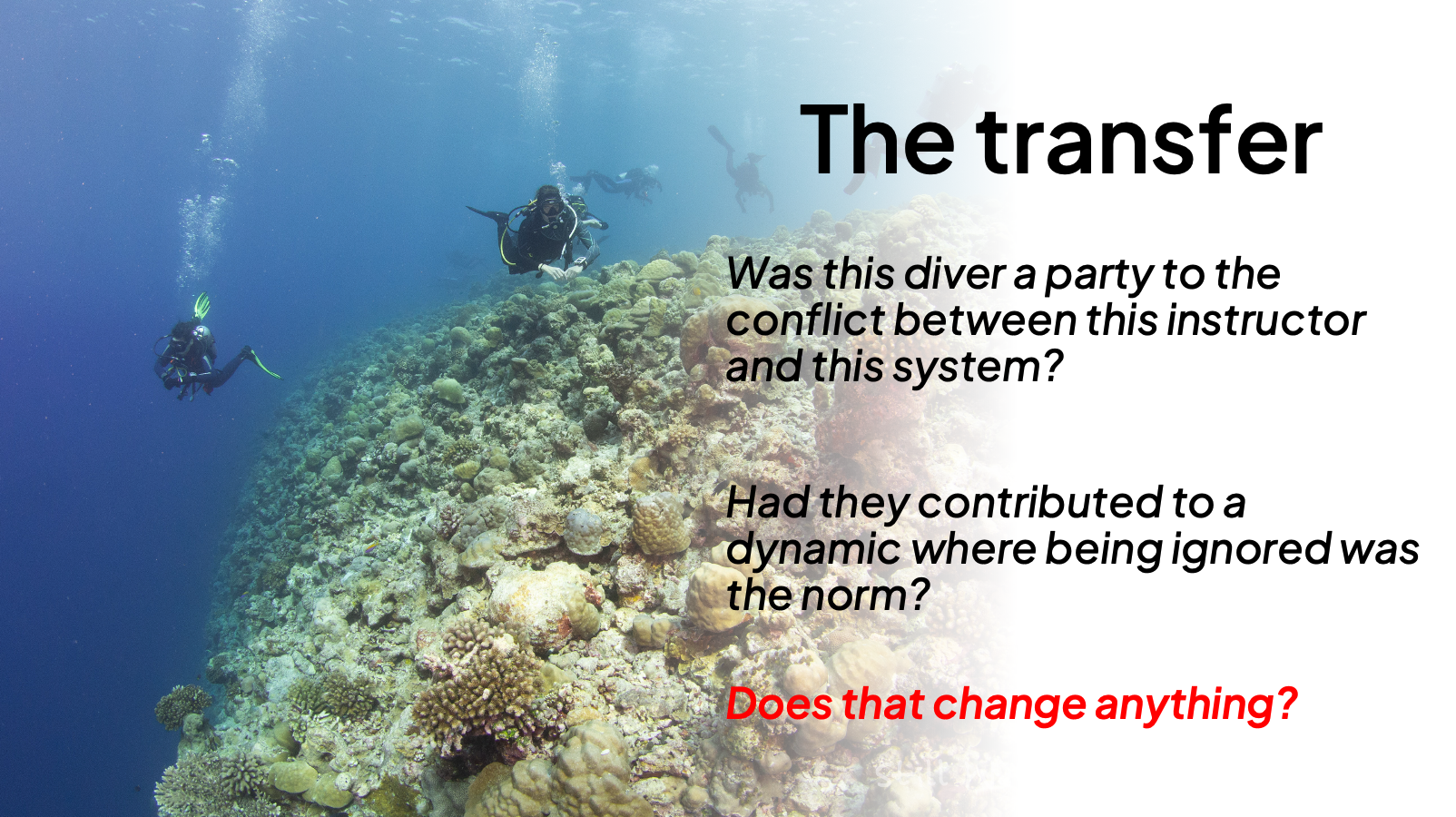
The diver had been informed of this. Repeatedly. He ignored professional advice, made his situation worse, and refused to cooperate with the person responsible for his safety. Was the instructor following the standard procedure — the very same procedure that the system had been applying to him for months? I told you. You didn’t listen. Now you’ll see why it matters.
How much does it cost
The operational cost of team erosion falls directly on the guests, who have no idea it even exists.
Decisions are made by people grappling with invisible cognitive deficits – resulting from chronic stress, recurring, unresolved conflicts and the constant effort not to say what they’re thinking. None of this will appear in the dive plan or in risk management.
Information stops circulating. Someone who knows that the equipment isn’t working properly doesn’t tell the new divemaster – because why bother, if nothing comes of it? The new divemaster takes a guest on a dive with equipment that he has no idea is faulty.
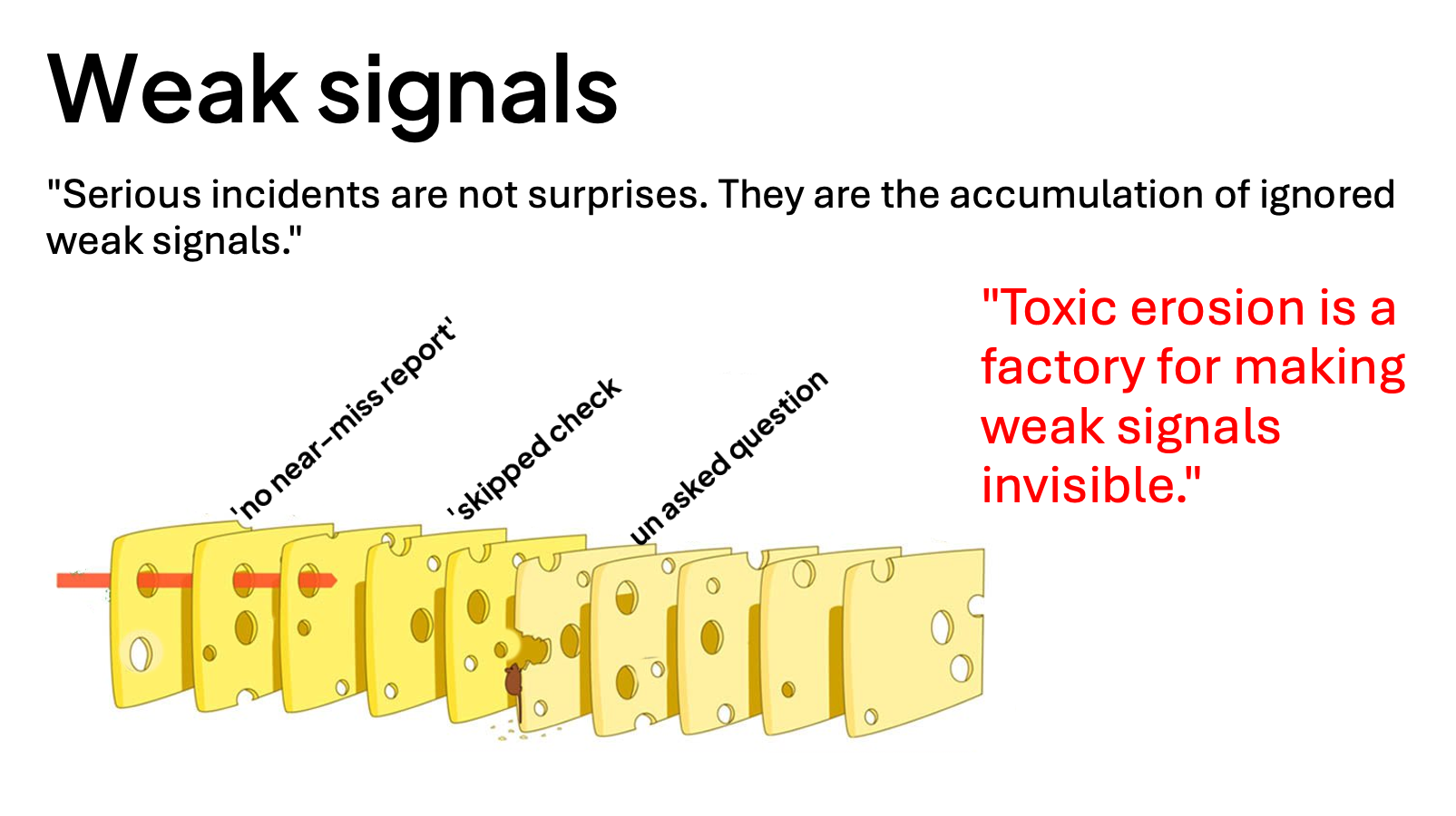
Potentially dangerous situations disappear. Not because they stop happening – but because the team has learnt that reporting them attracts attention without leading to any changes. The weak signals, which both James Reason and Karl Weick describe as precursors to serious incidents, are still there. The team has simply lost the ability to recognise them. Toxic erosion does not merely create risk. It creates a team that has lost the ability to recognise its own risk signals.
Two kinds of silence
In the briefing room, there are two kinds of silence that look completely different.
Silence born of fear is fraught with tension. Brief replies, avoidance of eye contact, hasty agreement, visible discomfort. Most human factors training focuses on this silence — and rightly so.
Silence born of resignation appears calm. The person nods. They say ‘all right’. They do not look tense, because they have stopped caring enough to get worked up about it. They are not afraid of the outcome. They are indifferent to it. This second kind of silence is far more dangerous, because it appears to be acceptance. And by the time it appears, the process of erosion is already well advanced.
Other points worth noting: do staff hold debriefings after dives, or do they operate solely in full view of guests? Could the most junior divemaster say, without any repercussions, ‘I’m too tired for this dive’? Are near-miss incidents discussed openly, or are they quietly swept under the carpet? Does the person carrying out the unseen maintenance work – the one who labels the tanks, checks the equipment thoroughly, and stays behind after hours to properly brief a difficult guest – know that their work is recognised?
When that person stops doing this – and eventually they will, if nothing changes – we’ll discover just how much our safety system relied on their unseen efforts. That’s a very bad time to find out.
For those who aren’t leaders: focus on observations, not on people. The phrase; ‘The trainee looked nervous before the dive’ opens the door; ‘you handled that badly’ closes it. Let’s ask about plans, not question decisions — a question cannot be brushed aside in the same way as an objection. Let’s document patterns, because feelings aren’t evidence, but dates are.
And for those working in a deeply toxic system where the leader is the source of the problem: the responsibility does not rest solely with you. Agencies, owners and certifying bodies bear structural responsibility for the environments they create and endorse. A culture of fair treatment, in its truest form, begins above the waterline.
The question that a culture of fair treatment has not yet answered
A culture of fair treatment provides us with the necessary language. Frontline staff should not be penalised for actions commensurate with their training and experience. Gross negligence, deliberate breaches and destructive acts are not tolerated.
The person who failed to fill the cylinder made a conscious decision. The instructor who failed to catch the bow line chose not to do so. The instructor who waited until the diver had descended to a depth of thirty-five metres — that decision was a conscious one. Under a strict interpretation of a ‘culture of fair treatment’, some of these cases fall on the wrong side of the line.
Can the system prompt deliberate action? Can an organisation — by ignoring its staff’s voices for months on end, by systematically eroding their sense of psychological safety, by repeatedly teaching its staff that the only effective form of communication is through consequences — lead to a situation for which a ‘culture of fair treatment’ holds an individual accountable?
This framework was designed to protect frontline staff from being blamed. And it is essential. However, applying it without questioning the conditions that shaped a particular behaviour amounts to treating the symptoms whilst leaving the causes untouched.
If someone reaches a point where allowing the system to collapse seems the only remaining form of agency, the question of what that system did to drive them to that point deserves at least as much attention as the act itself.
What are the causes of deliberate action? Where does gross negligence stem from? These questions do not negate individual responsibility. They add a layer that the diving safety community has not yet fully addressed.
Silence on the surface during a diving operation is never accidental.
It is an echo of everything that was silenced before anyone went underwater.
